Aug. 1, 2024

Malaria is one of our most ancient foes — and one of the wiliest.
Caused by parasites that certain mosquitoes spread through their bites, malaria overwhelms us, establishing an infection before we can put up a fight. It can go on to destroy red blood cells, batter organs, and even damage the brain.
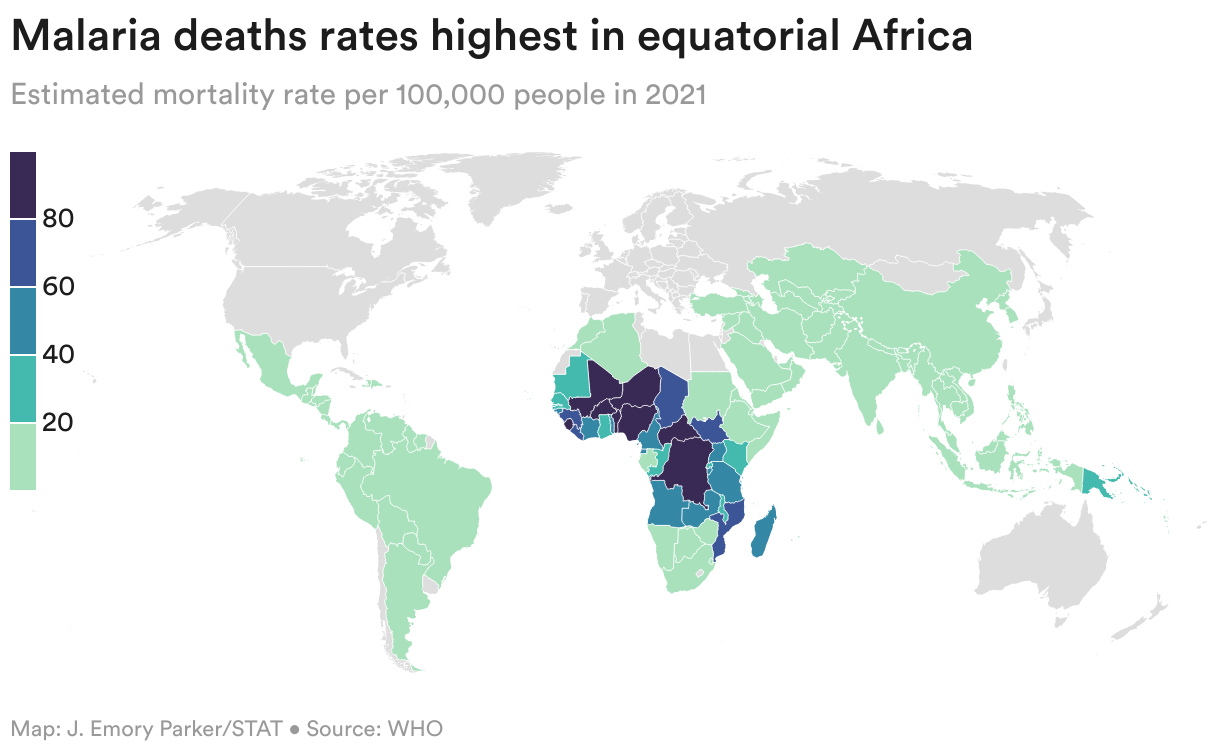
There are untold millions of cases, the vast majority of them in sub-Saharan Africa. Each year, hundreds of thousands of people die from the condition — some 80% of whom are children under 5. For decades, pharmaceutical companies and academic researchers have struggled to devise vaccines that could confer protection, fueling doubts whether such a product was even possible.
And yet, scientists have now succeeded. Twice over.
Earlier this year, routine immunization programs began rolling out a vaccine called RTS,S, reaching children in places including Cameroon, Sierra Leone, and Liberia. Last month, another shot, called R21, was introduced in South Sudan and Côte d’Ivoire, with more countries preparing campaigns for their youngest — and most vulnerable — citizens. RTS,S, also called Mosquirix, was developed by GSK and partners, while scientists at the University of Oxford built R21, which, based on the number of available doses alone, promises to be even more impactful.
Health officials have projected that the shots could save the lives of tens of thousands of kids. In some countries, malaria accounts for 25% of all childhood deaths.
The vaccines — the first to target any human parasite — represent a feat of both scientific grit and fundraising ingenuity. Researchers took on a sophisticated biological adversary that eludes our immune systems’ schemes to identify and dispatch it. They also had to find ways to nudge forward products that would never result in blockbuster sales, a reality that sapped much of the biopharma industry’s interest.
“We’re very fortunate, and when I say we I mean our generation, to be present for the last mile of this, and to see these vaccines be introduced,” said Eusebio Macete, a Mozambican researcher who two decades ago helped run an early trial of RTS,S. “And to see that one of the major killers in Africa could now have another tool to save lives, that’s amazing.”
The vaccines are by no means perfect, and given their limited effectiveness and durability, they are not the kinds of interventions expected to eliminate malaria in Africa. Rolling them out also poses huge challenges. The vaccines are given in four doses, starting around 5 months of age and ending over a year later with a booster, at intervals that don’t match when other childhood vaccines are administered. That means health workers must wrangle families to clinics or deliver vaccines to them in some of the globe’s most remote reaches.
The vaccines’ shortcomings have led some experts to argue against spending too much of the world’s resources on them instead of expanding existing measures, like insecticide-treated bed nets, mosquito control, and chemoprevention — that is, giving kids preventative drugs during peak transmission periods. As it is, only some 50% of kids sleep under bed nets in certain areas.
“We believe in the vaccine,” said Scott Filler, the head of malaria at the Global Fund, which helped support RTS,S. But, he said, prioritizing other strategies might offer more bang for the world’s buck. “Maybe we want to spend the world’s money first on these tried-and-true things, lay the foundation, and then start to deploy the vaccine in particular areas that have ongoing transmission, where kids continue to die,” he added.
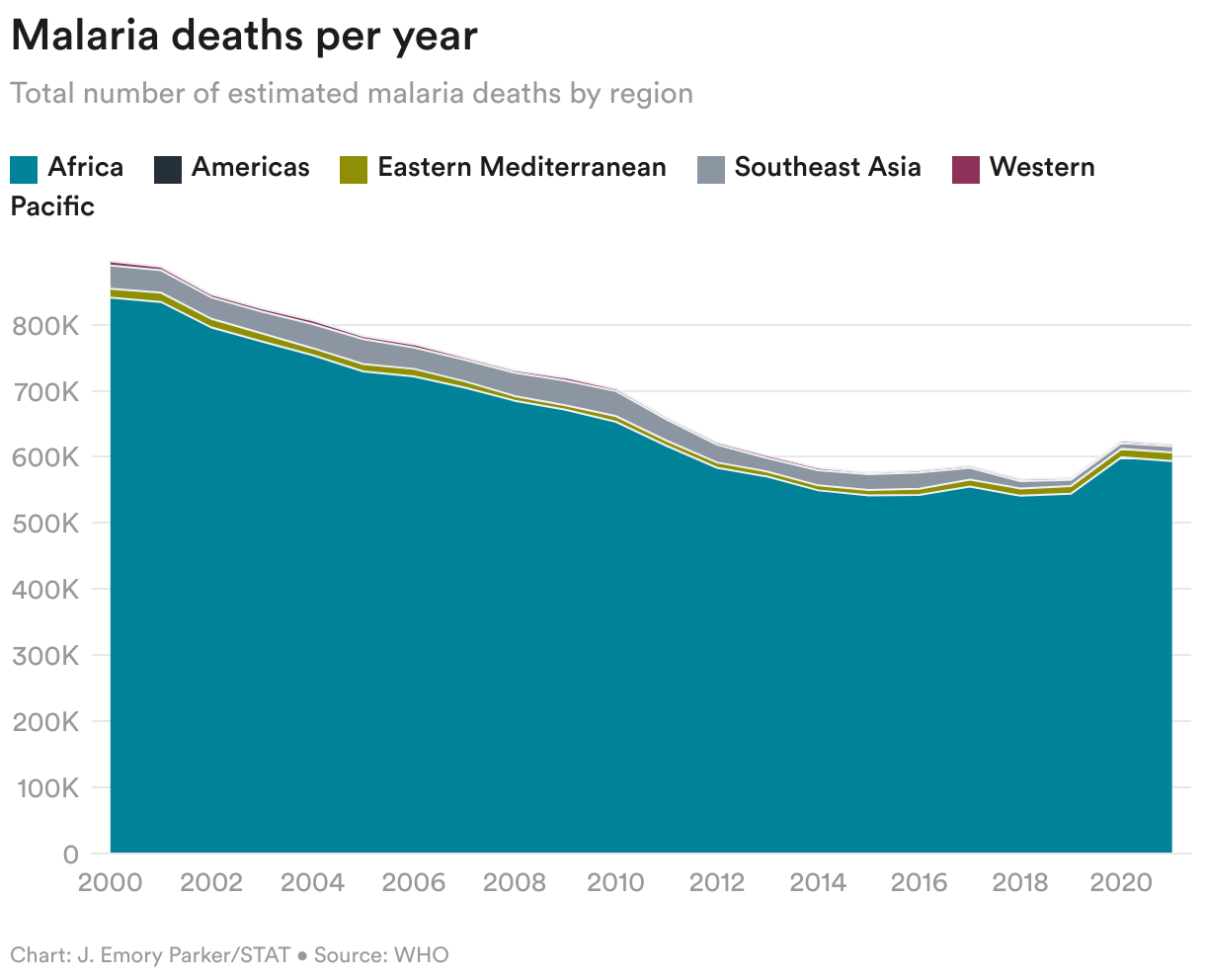
Other experts are more sanguine, even as they agree that the other interventions need to be maintained. They also argue that now is a particularly important time to take action. Progress against malaria has stalled, and after dropping to 576,000 in 2019, deaths caused by the disease have since surpassed 600,000 a year. Mosquitoes are becoming increasingly resistant to insecticides. The parasite that causes malaria is itself becoming increasingly resistant to medications. Climate change and migrating mosquito species are reshaping transmission zones.
“We’re at a crossroads,” Mary Hamel, the World Health Organization’s lead for malaria vaccines, told STAT. “We’re seeing cases go up in some places, and we have donors that maybe are not wanting to continue giving as much as they used to give. We’re in a period, I think, that’s precarious.”
This history of the malaria vaccines, an odyssey that stretches across decades and continents, is necessarily an abridged one. But it captures the achievement of how two vaccines reached the finish line within months of each other after more than 40 years of work. It’s one that relied on researchers willing to take on a mission that colleagues saw as quixotic, local investigators who pioneered running trials in their communities, and ultimately, the thousands of parents and children who volunteered for the studies — those who had most closely felt the ravages of malaria and enlisted in the global effort to neutralize one of the leading threats to children.
Ask experts for a good starting point to understand the history of the malaria vaccines, and one name comes up most often: Ruth Nussenzweig. Her work not only demonstrated the theoretical foundation of such a vaccine, but also helped uncover the bullseye that the shots target.
Twice an émigré, Ruth Sonntag was born in Vienna in 1928 into a Jewish family with physician parents. They escaped the Nazi occupation in 1938, eventually settling in Brazil. Her father urged her to become a nurse, thinking she would encounter less antisemitism in that role than as a doctor, but she saw medical school as a path to her real interest: research. It was while she was training at the University of São Paulo that she met another student, Victor Nussenzweig. “I was more interested in doing leftist politics than science, but I started dating Ruth and she convinced me that research would benefit people much more than politics,” Victor once told Science.
By then married, the couple headed to New York University for what they thought would be a brief fellowship for Victor but that turned into an academic home. A 1964 coup in Brazil brought in a period of strict military rule, upending their return.

While in Brazil, the Nussenzweigs had studied a parasitic infection called Chagas disease. By the time she got to NYU, Ruth had her eye on another parasite. Her aim was “always the same thing: develop a vaccine for malaria,” she said in an oral history for the university.
Designing a vaccine is not about attacking a bug directly. It’s about priming a person’s immune system to recognize and fight off a pathogen for itself.
But at the time the Nussenzweigs got to work, it wasn’t clear that that was possible with malaria. After all, there wasn’t a strong natural immune response that a vaccine could replicate. People did accrue some protection to malaria, but only after repeated infections, and it didn’t last all that long. It explained why people could be infected multiple times every year, and while older children and adults might build up enough armor to avoid getting seriously ill, young kids remained vulnerable to severe outcomes.
Nussenzweig, however, doubted the conventional wisdom. “The dogma at the time was that malaria doesn’t induce any immune response,” she said. “This was incorrect, and I knew it.”
She also proved it. In 1967, she and her colleagues showed they could protect mice from malaria by immunizing them with parasites that they had weakened with radiation. These parasites couldn’t cause disease, but they did, Nussenzweig found, elicit an immune response that staved off a future infection. That meant that, maybe, a vaccine could do the same.
Instead of using a whole bug to build a vaccine, which would be far more complicated, scientists often rely on an antigen, or a protein from the pathogen that provokes an immune response. The idea is that those generated immune fighters, namely antibodies, can then swarm invaders when they see the antigen in the form of an actual parasite.

But scientists faced a formidable challenge in identifying a suitable antigen from the malaria parasite, which is a much more complex intruder than the bacteria and viruses other vaccines target. Take the coronavirus that causes Covid-19. It has about a dozen genes, making the virus’s spike protein, which it uses to hack into cells, an obvious antigen to design vaccines around.
The malaria parasite has some 5,000 genes. Not only that, it has infected people for so many generations — our history dates back millions of years, to before we were even Homo sapiens — that it has evolved with us, essentially learning how to throw off our immune system’s defenses.
It gets more dizzying from there. Malaria doesn’t even look the same throughout its time in our bodies. When a female Anopheles mosquito bites us (males are vegetarian), she injects a bit of saliva to ensure the blood doesn’t clot as she takes her meal, which she needs to lay eggs. If she’s infected with the parasites, a few dozen of them will slip with the saliva into our skin. At that point, the parasites are squiggly critters called sporozoites.
Within about 30 minutes, the sporozoites are whisked via the bloodstream to the liver, where they multiply into the thousands over several days before busting out and invading red blood cells, triggering the classic symptoms of fever and chills and causing anemia.
With each infection phase, the parasite shapeshifts, with different genes activated and proteins expressed, becoming almost like a new creature. Any successful vaccine then would not only need the right bullseye, but be able to mount an immune response in the right place in the body, at the right stage of the infection.
Again, Nussenzweig came through. Once her earlier work showed that inducing immunity was possible, her team needed to identify which part of the parasite those elicited antibodies were recognizing — what could be a possible antigen. And together with her husband and other colleagues, she later zeroed in on a protein that surrounded the sporozoite. It became known, in the most scientifically sober way, as the circumsporozoite protein, or CSP. (Other research teams contributed key discoveries around this time.)
That finding became the blueprint for the vaccines. The question was, could you design a shot based on CSP as your antigen, building up an army of anti-CSP antibodies? And could those antibodies then block any injected parasites from making it to the liver, preventing an infection from taking hold?
Ruth Nussenzweig died in 2018 at 89, and Victor, now in his mid-90s, is so hard of hearing that an interview was not feasible, said their son Michel Nussenzweig, himself a scientist at Rockefeller University. But it seemed the couple knew their work might one day result in a breakthrough.
“It is therefore conceivable that a vaccine containing only sporozoite antigens would completely protect a portion of the exposed population,” they wrote in one review.
They authored that paper in 1984. Another 40 years of work remained.

When Ripley Ballou’s fever struck, he first thought that he was reacting to the home-brewed beer he had tried at a friend’s party. But as he got sicker, he realized what was actually happening: He had given himself malaria. It also meant his experimental vaccine hadn’t worked.
Ballou, who goes by Rip, was a physician at the Walter Reed Army Institute of Research helping lead a team whose task was to turn the antigen the Nussenzweigs had identified into an actual product. The Army, keen for a vaccine that could protect soldiers, selected a company called Smith, Kline & French as its development partner, striking a collaboration with the GSK precursor in 1984. Their particular target became Plasmodium falciparum — the deadliest form of the malaria parasite, and the one that dominates in sub-Saharan Africa.
When the researchers had their first candidate ready to test, Ballou rallied colleagues to join him in rolling up their sleeves for a challenge study, in which volunteers receive an experimental vaccination, then expose themselves to a pathogen to assess if it worked. (In these tests, the military used a malaria strain they knew was treatable.)
Once Ballou and his comrades got the vaccine, it was mosquito munch time. They pressed gauze-covered cups containing infected mosquitoes against their arms, offering up a blood buffet. Days later, Ballou got sick. So did four others. One person, however, did not.
It was by no means a good result, but it was an important one. “That basically showed us it could be done, that it was possible” for a vaccine to block an infection, Ballou said. But for it to be workable, they would need to show much higher rates of protection.
The team spent the next decade refining the vaccine. There are different ways to present an antigen to the immune system, so they tinkered and toiled in hopes of landing on an approach that could stimulate a response so robust as to be protective. They combined the CSP antigen with genes from other pathogens, and turned to proteins used in other vaccines, and made chains of bits of proteins, all in hopes of whipping up a phalanx of antibodies.
And it just wasn’t working.
“We probably did eight or nine challenge trials where nearly everyone had malaria,” Ballou recalled. They even ran out of friends they could rely on at Walter Reed for the studies, so had to recruit in the local community.
Part of the problem may have been that their experimental vaccines weren’t conjuring up the sky-high antibody levels needed to fend off malaria — much higher than the levels needed to protect against many bacteria and viruses, given that the parasites are so good at evading our defenses.
The antibodies also have to be quite the hunters. To stave off an infection, the immune guardians have to clear out all the injected sporozoites before they make it to the liver. While some scientists say that the more sporozoites that reach the liver, the more likely someone is to get sick, others stress that if even one infiltrates a liver cell and starts replicating, it can turn into a full-blown infection. Imagine a teenager cleaning up from the party he threw with his parents out of town — overlooking even one cup could land him in trouble.
“To say it was a discouraging period does not quite capture the feeling,” Ballou, who is now at the infectious diseases nonprofit IAVI, wrote in 2009 about the failed attempts.
But more than 3,000 miles away, a scientist had an idea.

Before Joe Cohen became a researcher, his jobs included working in a fabric store’s stockroom and analyzing stool samples at a hospital lab.
Cohen was born in Egypt and, when he moved with his mother to France in 1962 after finishing high school, he halted his studies to support his family. He eventually made it to university, where he focused on agricultural engineering. But really, it was the nascent molecular biology field that caught his eye.
He then joined other relatives who had moved to the United States, but he didn’t know how to apply to doctorate programs. He simply showed up at nearby Brooklyn College one day and introduced himself. He was admitted.
When Cohen was wrapping up his training, he struggled to find an academic job that suited him. But he spotted an ad — he can’t remember if it was in Nature or Science — from Smith, Kline & French in Belgium looking for a molecular biologist with experience in yeast genetics. “That essentially described me,” he said.
It wasn’t academia, but he admired the group’s innovative work on a hepatitis B vaccine in development at the time. So he moved his wife, infant daughter, and aging mutt named Clebs to Belgium in 1984, joining the team right as it was wrapping up its hepatitis B work. It was his first non-trainee job in science, at age 40.
A few years later, Cohen’s bosses asked him to take the lead on the malaria project, which the company was transferring from its U.S. labs to Belgium. Other colleagues had already said no to the assignment, Cohen recalled, thinking it was a lost cause.
Cohen didn’t have much experience with parasites, but the scientific challenge appealed to him. So did the impact he might have if the team succeeded. And in taking on the project, he drew inspiration from the hepatitis B vaccine.
GSK scientists had created that shot by engineering yeast cells to express one of the virus’s proteins, which they had identified could act as an antigen. When researchers would crack open the cells, the proteins would spontaneously glom onto each other, forming what’s called a virus-like particle. The vaccine was made of schools of those particles.
What if, Cohen thought, you could just add CSP — the malaria antigen — into the mix?
Cohen grinded away in the lab, into the night, on weekends, on holidays. By linking genes from the hepatitis B virus and the malaria parasite, he was able to express what are known as fusion proteins in the yeast cells — meaning they had antigens from both pathogens — that he still got to ball together into virus-like particles. They looked like blobs encircled by a coating of hepatitis B antigens, and then, jutting out from the surface, like cloves studding an orange, were the malaria antigens.
The theory was that by presenting the body with a virus-like particle — which resembled a virus in both size and shape — the immune system was going to generate a heartier response than it would when presented with just a bit of the protein itself. After all, the immune system knows what to do when it sees something that looks like a virus.
As it happened, other GSK scientists were building up another branch of vaccine research. They were designing a line of adjuvants, which boost the power of a vaccine by deepening the immune response. Researchers started testing the malaria shot in combination with a number of the adjuvants.
Then, finally, came the challenge study of the vaccine with an adjuvant called AS02.
Ballou was in his kitchen when he got the call: Six of seven volunteers had been protected, as the scientists reported in the New England Journal of Medicine in early 1997.
The vaccine, dubbed RTS,S, had worked. It was time to test it in the field.


One of the team’s early calls was to a researcher named Brian Greenwood. Greenwood had already proven the power of insecticide-treated bed nets, but he believed in vaccines, even as other experts dismissed them. Greenwood once even made a bet with another senior scientist — whom he declined to name — about whether the world would ever see a malaria vaccine.
Greenwood, who is British, was running a research site in the Gambia. He had previously worked on a study in Tanzania of a vaccine candidate developed by a Colombian scientist named Manuel Patarroyo, and while that shot ultimately fizzled out, the experience left Greenwood with a lesson. “It taught us how to do a malaria vaccine trial,” he said.
Greenwood and colleagues started recruiting a cohort of men to evaluate RTS,S, with some receiving the experimental shot and some getting a rabies vaccine as the control. At the time, the researchers thought a highly effective vaccine could still be used for adults. Plus, it’s considered unethical to test a vaccine in children before its safety is established in older volunteers.
The results, published in 2001, were a bit of a bust. The shots showed some protection, but it wasn’t very strong and waned quickly. As Ballou wrote in a review, “the vaccine was still clearly not sufficiently efficacious to support its further development as a stand-alone vaccine for travelers or the military.”
But the adult trial furthered the researchers’ belief that the shot had pediatric potential. They reasoned that if the vaccine reduced the risk of malaria to an extent in adults, it was likely to be even more protective in kids, who tend to mount stronger immune responses to vaccines.
The prospect of healthy returns had evaporated, however. A company could never charge much for a product whose only takers would be children in some of the world’s poorest countries. Wealthy tourists and the Defense Department they were not.
GSK brass allowed the team to continue with the program, but there was a catch: The company would no longer fund the project without others’ support.
It was a key inflection point, one that underscores how commercial realities shape the programs drugmakers pursue or scuttle. It’s not just the programs companies back, either. With potentially lucrative products, companies start planning future trials and scaling manufacturing at risk even before the prior step in the development gauntlet is complete, all to expedite the process. With neglected disease products, it’s likely that no one is going to put up the money for the next study until it’s clear that it’s going to happen, a factor that dragged out the timeframe of the malaria vaccines.
Public health experts credit GSK for sticking with the malaria program at all, particularly given its daunting nature, and say it’s unclear whether other companies would have done the same. Thomas Breuer, GSK’s chief global health officer, said in an interview with STAT that the company has covered the “lion’s share” of funding for RTS,S throughout its development, at more than $700 million.
While GSK has faced recent criticism for how it’s handled the development of a tuberculosis vaccine, Breuer said that the drugmaker sees a need to partner on these products, not just to share the financial risk, but because the company doesn’t have all the relevant expertise itself. He stressed that GSK continues to invest in global health.
“We have a social responsibility, and this was not just true for the malaria vaccine,” he said, citing the company’s development work in other neglected diseases. But, he added, “Even GSK, who is committed in the long run, cannot fund all the activities.”
Luckily, another funding model was emerging around that time. The Bill & Melinda Gates Foundation, established in 2000, had started backing a nonprofit called PATH and its Malaria Vaccine Initiative. And in 2001, GSK and PATH struck a partnership to push RTS,S forward. In total, said Helen Jamet, a malaria official at the Gates Foundation, the organization put $200 million into RTS,S, primarily through PATH’s work.
With that partnership in place, researchers moved to test the vaccine in kids. For the site, they selected Centro de Investigação em Saúde in Manhiça, Mozambique, which Spanish experts had helped start, but, crucially, was staffed largely by local providers. The team set out to recruit parents in the community to enroll their children in the study, setting aside time to talk with them about the vaccine and address their questions.
It helped that parents were well aware of the risks posed by malaria. Children would get sick two, five, eight times a year. Kids would miss school, and parents would miss work to care for them. At hospitals, where even now a third of consultations in some regions are tied to malaria, bags of blood being readied for transfusions would line the walls. Clinics would be so full that three children would share a bed, all pale and flopped over and breathing shallowly.
Laurinda Carlos Balate was one of the moms who said yes to the study. Some of her friends didn’t understand why, and told her the experimental shot might be dangerous. But she liked the idea of combating malaria, and she trusted the clinic’s staff.
“I’m quite happy, because the vaccine was a success,” she said recently over Zoom.
Her daughter, Loyde Carina Nhabanga, who was just a baby when her mother enrolled her in the study, now has a 7-month-old of her own, whom she said she is planning on getting vaccinated when the shots become available. “It’s going to help us fight against malaria,” she said.
Overall, the Phase 2 trial, run in 2,000 children, showed the vaccine was 30% effective at preventing malaria, and 58% effective at protecting against severe malaria, according to findings published in 2004. It was the first sign that the vaccine could generate a protective response in kids in high-transmission areas.
Other studies of RTS,S showed similar outcomes, building evidence that was promising enough to move the shot into a pivotal Phase 3 trial. (During this series of trials, the researchers switched the adjuvant from AS02 to one called AS01 that prompted stronger immune responses. AS01 is also used in GSK’s RSV and shingles vaccines.)
It was around this time that researchers in England came up with their own vaccine candidate.
Adrian Hill came to malaria vaccines through a circuitous route. Hill, now the director of the University of Oxford’s Jenner Institute, had trained as a geneticist, studying how different genetic variants that had evolved in certain communities made people less vulnerable to malaria. (If the legacy of malaria is written in our history books — it may have killed Alexander the Great, Genghis Khan, and a couple of popes — it is also imprinted in our DNA.)

It was when Hill was studying one of those variants in the Gambia in the 1980s that he got an up-close look at the parasite’s toll. Children were packed into a clinic, arriving so sick they desperately needed blood transfusions. So he pivoted.
“That kind of converted me from thinking, we’ve got to really understand susceptibility to malaria, to thinking, what’s going on with vaccines?” he said in an interview at his Oxford office.
Starting in the 1990s, Hill and his colleagues threw a number of strategies at malaria. They tried DNA-based vaccines and viral vector vaccines — like the one Oxford researchers would later develop with AstraZeneca against Covid-19 — and different combinations of those different kinds of vaccines, without much success.
But they also thought of updating RTS,S. After all, by the early 2010s, some two decades of advances in research methods — including in expressing proteins in yeast — had accrued since the early days of the GSK shot. “Making the vaccine 25 years later helped us,” Hill said.
The issue with RTS,S, at least as far as Hill and his colleagues believed, was that there wasn’t enough malaria antigen on the particle versus hepatitis B antigen. They hypothesized that if they could engineer both a greater amount and higher density of the former, the particle would elicit a more powerful anti-malaria immune response, with more antibodies produced that were even sharper at targeting sporozoites. They essentially wanted to stud more cloves onto the orange.
The task of figuring it out fell to a graduate student named Katharine Collins. The potential trip-up was that if the Oxford researchers increased the amount of malaria antigen in their recipe, the proteins wouldn’t self-assemble into a virus-like particle, which was crucial to generating an actionable immune response. Whether or not proteins arrange into that kind of particle depends on a delicate balance of chemical charges, with the right bonds needed to form for it to be a stable molecule.

It took some trial and error, but by refining the process, Collins made it happen. “I would express the protein in the yeast, bust them open, do a really simple purification, and then go and have a look under an electron microscope,” said Collins, who now works at the charity Open Philanthropy. “And we saw particles. It was like, ‘wow.’”
For their adjuvant, the Oxford team landed on one called Matrix-M from Novavax, which is now used in that company’s Covid jab. The shot became known as R21.
But like RTS,S, R21 ran into funding issues. When it came time to manufacture doses for human trials, Hill turned to Oxford’s own production site, which was cheaper than a contract manufacturer. But with limited resources and know-how, the team struggled to make the vaccine at scale. From the promising lab experiments to having doses for a challenge trial, three years would pass.


When data from the Phase 3 trial of RTS,S arrived, the reaction was lukewarm.
The trial, which ran from 2009 to 2014, enrolled nearly 9,000 children from 5 months to 17 months of age in seven countries, places where malaria circulated year-round as well as places with seasonal transmission. While the initial protection appeared strong, the efficacy dropped to between 30% and 50%. Adjectives like “modest” and “moderate” were thrown around.
Some experts excavated a rosier view. Given the scope of the disease, they argued, preventing even a third of malaria cases would have major repercussions for health systems, economies, and families.
“Because of the sheer number of cases of malaria — there are hundreds of millions of cases of malaria every year — what we saw was that in some of the areas where the intensity of malaria transmission was higher, where children got more malaria, we saw over 6,000 cases of malaria prevented for every thousand children vaccinated,” said Ashley Birkett, a longtime PATH official.
But another issue arose — potential safety signals with the vaccine. One was that there were more cases of meningitis, an inflammation around the brain and spinal cord, among children who received RTS,S than those who got the control shots.
It was up to regulators to weigh in. The European Medicines Agency gave the vaccine a positive review in 2015, but it was a WHO recommendation that mattered most. The global agency needs to give its stamp of approval if groups like UNICEF and Gavi, an international organization known as the Vaccine Alliance, which help purchase immunizations and deliver them to low-income countries, are going to add a shot to the portfolio of products they provide.
The WHO’s advisers weren’t overly enthusiastic. Based on the data, the vaccine didn’t seem like a game-changing intervention. With the potential safety issue, they worried not only that introducing the vaccine might lead to meningitis cases, but that moving too quickly could turn people against other immunizations.
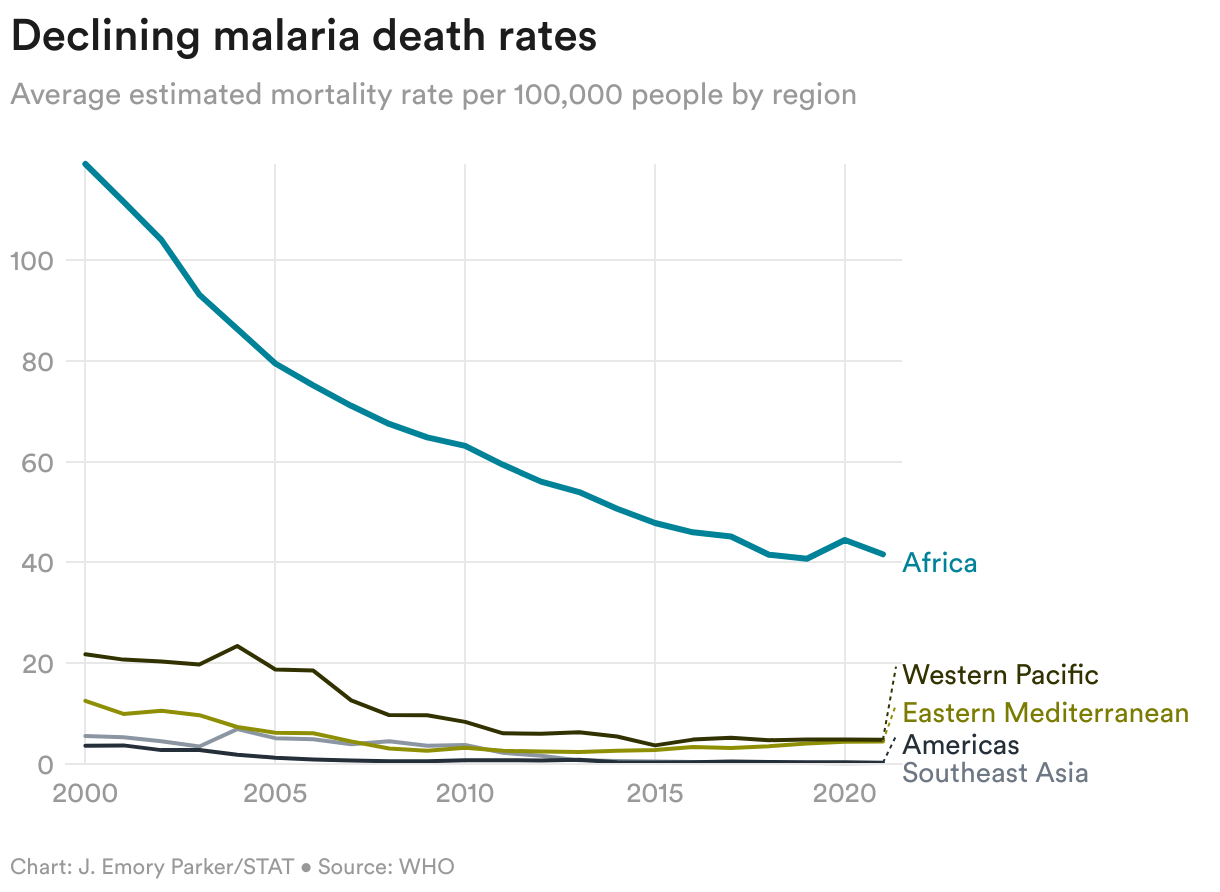
The context of the moment also shaped experts’ thinking, those involved at the time recalled in recent interviews. The world had been making steady progress against malaria, with cases cut by 27% from 2000 to 2015. No one foresaw that tide reversing.
“There was not a sense that we desperately needed a vaccine, let alone a vaccine with modest efficacy,” said Pedro Alonso, who directed WHO’s malaria program at the time.
Instead of recommending the vaccine, the WHO in 2016 decided to push forward with a pilot program, which would involve deploying millions of doses to children in three countries. The move was seen as a compromise — the agency was not spurning the vaccine, but it wasn’t endorsing its wide rollout either. The program would also provide the chance for experts to assess the feasibility of using the vaccine outside a trial. Would people get their children to a clinic for four doses? Would they give up other safeguards against malaria?
But if the pilot made sense as a way of shoring up the vaccine’s evidence, it created a new challenge, one that some experts worried could jeopardize the shot. As Birkett said, “Nobody was anticipating the pilot program. Nobody had the money ready to go.”
The Gates Foundation by that point had pulled back from putting more funding into RTS,S, but the WHO scrounged $70 million for the pilot from sources including Unitaid, Gavi, and the Global Fund, with doses donated by GSK. But the time needed to fundraise and plan, including getting the three selected countries — Ghana, Malawi, and Kenya — on board, meant shots didn’t start being administered until 2019, three years after the pilot was decided on.
Once underway, it became clear that the meningitis issue was a statistical fluke from the trial — that there was no real safety issue. And in 2021, the WHO endorsed RTS,S as the world’s first malaria vaccine.
Ultimately, the pilot program demonstrated not only that RTS,S could be reliably rolled out, but that even with its modest efficacy, it could have sweeping impacts. It didn’t lead to drops in other vaccinations. Families kept up with other anti-malaria interventions. And it cut childhood mortality broadly by more than 10%, a sign, perhaps, of how malaria infections leave children vulnerable to other illnesses. Places where the shots were deployed saw malaria hospitalizations cut by a fifth.
“These numbers are huge,” said Kwaku Poku Asante, the director of Ghana’s Kintampo Health Research Centre and an investigator in the pilot program. “If you sit in a district hospital, where every child has malaria, and all of a sudden you’re seeing a reduction by one-fifth, that is huge.”
Some experts maintain the pilot program was necessary — that a wide-scale rollout would not have succeeded had WHO recommended RTS,S in 2016. But in hindsight, others are more conflicted. They find themselves wrestling with the decision, wondering if the vaccine had been put into use then, instead of years later, how many more thousands of children might have been saved?
“This has haunted me for a number of years. The question is, did we do the right thing, or did we not?” said Alonso, now at the University of Barcelona. “I do often think of the costs.”


After a successful challenge trial and safety tests, it was time for the Oxford team to try R21 in the field. They scraped together funding from sources including the Wellcome Trust and the European and Developing Countries Clinical Trials Partnership, and in 2019 launched a Phase 2 trial in children from 5 months to 17 months of age in Nanoro, Burkina Faso.
The results surpassed their hopes. The shot showed about 75% efficacy.
“We were expecting in the best case scenario 60% efficacy or something like that,” said Halidou Tinto, who leads the clinical research unit in Nanoro. “And then we were at almost 80%. This was a big surprise, but a very nice surprise.”
For the Phase 3 study, instead of the Oxford team having to pitch companies to fund the research, a partner came to them. One day in 2017, a man named Umesh Shaligram showed up at Hill’s office. Shaligram was a top scientist at the Serum Institute of India, the world’s largest vaccine manufacturer. The institute had heard about Oxford’s promising data, he told Hill, and was curious to learn more.
With the resulting pact between Oxford and Serum, not only did Serum start manufacturing R21, it even funded the Phase 3 trial, a study of 5,000 children in four countries run in 2021 and 2022. The vaccine showed about 70% efficacy.
Last October, the WHO recommended the vaccine.

A few months ago, a package arrived for Brian Greenwood, the old malaria hand who had helped run the early RTS,S trial in the Gambia. It contained six “very nice” bottles of red wine. The other expert with whom Greenwood had made a bet about the feasibility of a malaria vaccine was making good after losing that decades-old wager.
The bottles’ arrival coincided with the rollout of RTS,S in Cameroon in January, the first time a malaria shot was deployed in a routine immunization program. More countries will launch their own vaccination campaigns in the coming months.
Experts debate whether one vaccine is superior to the other. Many favor R21, pointing to its updated design and the higher efficacy scores it reached in trials. Others counter that the differences in the trials — including the timing of the doses relative to peak transmission periods — render comparisons impossible. The WHO has taken to saying that both shots can reduce malaria cases by about 75% when given before peak transmission periods and combined with other interventions.
“The important thing now is to get the vaccines used,” said Greenwood, who worked on studies of both shots and is now at the London School of Hygiene & Tropical Medicine.
R21 does have some inarguable advantages. While manufacturing is still being scaled up, thanks to the partnership with the Serum Institute, 100 million doses could be produced a year, at a cost of $2 to $4 per dose. GSK, meanwhile, is only producing 18 million RTS,S doses from 2023 to 2025, at an approximate cost of $10 per dose, and then committing 15 million doses a year from 2026 to 2028. The company is transferring the vaccine to Bharat Biotech, another large Indian manufacturer, which should result in more doses at a lower cost, but it’s expected that the Bharat facility won’t be supplying RTS,S until 2028.
The vaccines are important in other ways. They established how to run clinical studies, built up trial infrastructures, and gave regulators experience evaluating malaria shots. Even with the financial challenges it faced, R21, with its strong data profile, comparatively breezed through its studies and regulatory reviews, winning approval faster than many experts anticipated. Future vaccines could have an even more streamlined route.
And next-generation vaccines are coming. Some target different life stages of the parasite, so could be combined with a shot like R21. Some could protect adults — including, crucially, during pregnancy, a time when a malaria infection is dangerous to both mother and baby. They could have higher efficacy, greater durability, and even halt transmission — the type of tool that could make eradication a prospect.
In that way, then, RTS,S and R21 have another legacy. They showed that a malaria vaccine was possible.
About the Author
To submit a correction request, please visit our Contact Us page.





