
STAT teamed up with Word In Black, a network of 10 Black news publishers, to report over the past year on the impact of new weight loss drugs on Black America.
Jonathan Gustave was diagnosed with type 2 diabetes last August after decades of struggling with his weight. To help lower his blood sugar levels, his doctor prescribed Ozempic, the diabetes drug that has become wildly popular for its weight loss effects.
The drug was in such demand that Gustave, a 38-year-old Orlando, Fla., resident, had to wait two months for the pharmacy to fill his prescription. A month and a half later, he ran out, and another two months passed before the pharmacy would give him a refill, and only for six months.
GLP-1 drugs, a class that includes Ozempic, are transforming the treatment of diabetes and obesity. Studies have been finding they have benefits for heart health and other conditions, too. But many Black Americans, including patients like Gustave and medical experts, worry that their community is being left behind. They say, too, that the public’s obsession with the drugs serves as a reminder of how Black bodies are policed and judged by society.
“I do feel like Black people face more barriers because it all depends on what type of health insurance you have,” Gustave said. “I know a lot of people who forgo health insurance to have more money on hand to pay bills. If you don’t have insurance, or good insurance, it’s going to be more challenging to access it.”
Black Americans have long had higher than average rates of chronic disease, for reasons that include disparities in income and education; less access to health insurance, housing, healthy food; and the “weathering” of racism-related stress. According to federal health data, 12% of non-Hispanic Black adults had diagnosed diabetes in 2021, a rate surpassed only by American Indians and Alaska Natives; non-Hispanic Black adults have the highest rates of obesity, based on body mass index, at nearly 50%. Recent studies, though, found that Black people with diabetes are less likely to be prescribed GLP-1 drugs.
Calvin Smith, assistant professor and clerkship director for internal medicine at Meharry Medical College, said he’s seen a lot of inequities in how Black and Hispanic patients are treated when trying to access the GLP-1s despite their greater burden of obesity and diabetes.
“In an ideal situation, they should be receiving these medications at a rate that is more commensurate with the incidence of it,” he said.
Mopelola Adeyemo, an endocrinologist and assistant professor in the department of medicine in the division of clinical nutrition at UCLA, said that more and more of her patients have been asking for the new weight loss drugs, many of them concerned about lockdown weight gain during Covid. But oftentimes, she said, they are unaware that there are side effects and that the expensive drugs need to be taken indefinitely to retain any weight loss.
“I think providers and researchers need to keep an eye on if we are going to see a disproportionate burden of obesity, diabetes, and heart disease later on because of a disparity in prescribing these medications,” she said.


Left out of the conversation
The new GLP-1 drugs, most of them taken by weekly injections, mimic the effect of hormones triggered by food and tend to slow down digestion and curb hunger. Soon after Ozempic was approved by the Food and Drug Administration in 2017 to treat diabetes, it started getting used off-label for anyone looking to lose weight — regardless of their diabetes status.
Novo Nordisk now sells semaglutide, the same active ingredient in Ozempic, as Wegovy for obesity, and last year, it took in more than $18 billion in sales from the two drugs. Eli Lilly, meanwhile, sells a potent GLP-1 based drug, tirzepatide, as Mounjaro for diabetes and Zepbound for obesity; sales hit $2.4 billion last year. All four drugs have been in shortage at various times in the last year.
Accessing the drugs largely depends on insurance status, the ability to pay out-of-pocket costs, and whether a pharmacy has it in stock. Without insurance or if prescribed off-label, Ozempic has a list price of $935.77 for the three different pen dosages of 0.25 to 2.0 milligrams.
Fatima Cody Stanford, an obesity medicine physician-scientist at Massachusetts General Hospital, has tracked the nation’s obsession with weight loss over her 20 years as a physician. With the new era of anti-obesity medications, the lines between who has access to it and who doesn’t continue to be defined.
“I think the conversation is definitely missing the Black community,” said Stanford, who has consulted with companies that make GLP-1s. “We hear the privileged white voice in the community because that’s usually who can afford it and who gets the access and care.”
She noted that medical spas are administering compounded versions of semaglutide and warned that they may not be safe. “We’ve gotten into a situation with the shortages where people feel like they can do whatever they want,” she said. “It’s like the wild, wild west out here.”
In September 2023, Timothy Conley got an ultimatum from his doctor — it’s either Ozempic or surgery. Conley, who is department chair for cinema at California College of ASU, describes himself as addicted to fast food and has tried dozens of diets and medications to manage his type 2 diabetes and weight.
He opted for the medication.
After a six-week wait for a supply, he started Ozempic in mid-October — and shortly after, the side effects hit. Initially, it was just nausea and stomachaches, which quickly turned into rough bouts of diarrhea. Every Monday, he takes the weekly shot, and so far, it helps curb his cravings. But what’s hard for him is only being able to eat small amounts of food — and feeling hungry shortly afterward.
“Four days ago, I felt this hunger at 10 o’clock at night. I ate a protein bar. But something in that protein bar caused my stomach to go into this crazy space where I started having diarrhea,” Conley said. “It affects my livelihood in the sense that I’m up until two or three in the morning trying to figure this out.”
Smith noted that bodies react differently to the medications. Not everyone responds, and many people, he said, don’t realize that anti-obesity medications typically only cause 5% to 15% of body fat loss. The drugs have been hyped as a quick fix, but Smith stressed that they are for long-term use and that each person needs to discuss the risks and side effects with their doctors.
Adeyemo, the UCLA clinical nutritionist, was blunt: “There is no miracle drug,” she said. “The idea that this is a miracle fix to obesity … is not accurate. Obesity is a chronic problem.”
Weight bias plus racial bias
Living with obesity has commonly been seen as a choice and moral failure. A 2019 journal article, “The Moralization of Obesity,” points out that weight stigma is pervasive in American culture and observes, “Associations of obesity with disgust and poor moral character (e.g., laziness) suggest that people may view obesity as a violation of bodily purity, a highly moralized domain.”
In the last few years, Stanford said she’s seen a shift in public perception of obesity, with more people recognizing it as a disease. But for Black folks living with obesity, not only do they continue to face weight bias, but they also face racial bias. “Unfortunately, obesity is a disease that you wear,” she said, and with that comes conceptions about who you are, your value, and your worth.
The debate about who should use GLP-1 drugs — or not — continues to flare as more celebrities acknowledge using them. In December, Oprah Winfrey, one of the most high-profile Black celebrities of our time, revealed she used one of the new obesity drugs to lose weight and followed that up in March with a one-hour special, “Shame, Blame and the Weight Loss Revolution.” The criticism that followed suggests that Americans are still at odds over the moral case for these drugs.
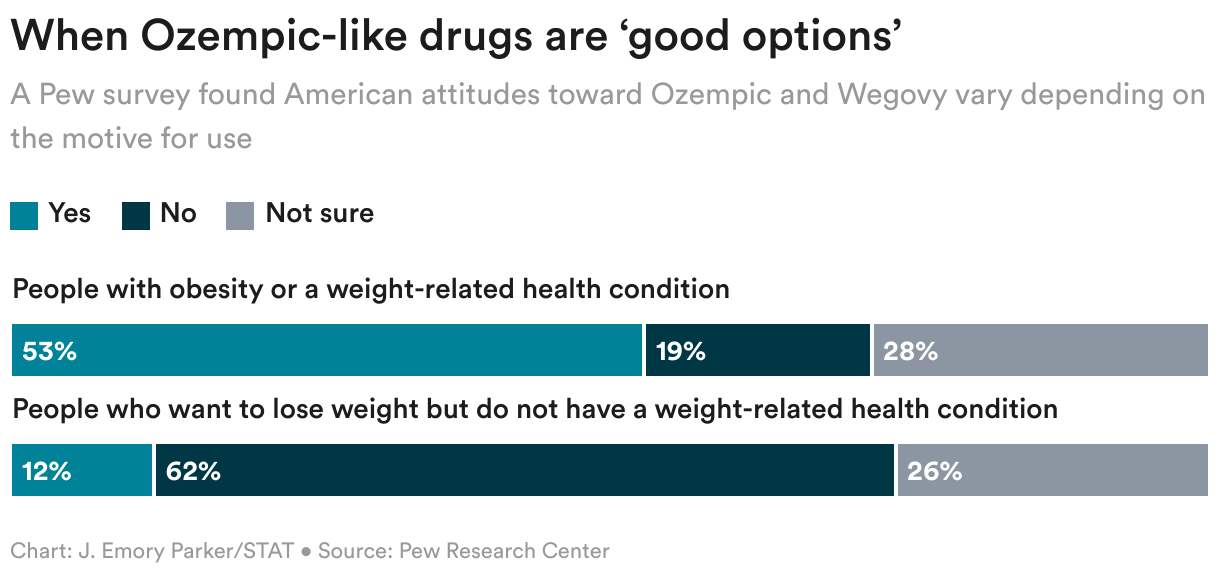
In a Pew Research Center survey this year of U.S. adults, 53% of Americans who had heard of drugs like Ozempic saw them as a good weight loss option for people who have obesity or a weight-related condition, while only 12% saw it as a good option for people who want to lose weight but don’t have a related health condition.
The medical field is often at the epicenter of weight shame and medical dismissal. In a study of physician attitudes toward patients living with obesity, doctors were more likely to rate the encounter as a waste of time and would spend less time than with a patient without obesity. Without proper evaluation, physicians often blame a patient’s symptoms on obesity.
“With obesity, we do blame people because we think … the right way is diet and exercise,” Stanford said of the backlash people get for undergoing surgery or taking weight loss medications. “We have this moral code that we espouse that people have to use.”
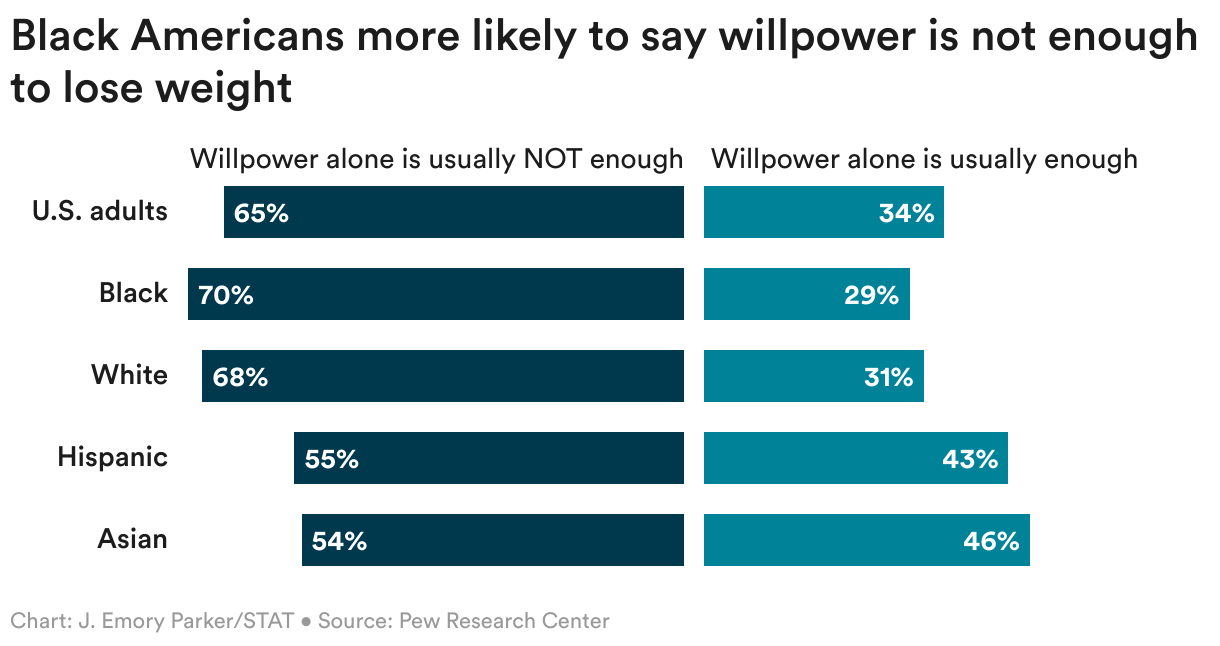
In a society in which some health care professionals dismiss patients living with obesity, it’s not a surprise that many Americans believe a strict diet and exercise regimen is enough to lose weight. Yet in the Pew survey, 70% of Black Americans said willpower alone is not enough to lose weight and keep it off.
“We are not lazy Black people. We care about our disease,” Stanford said. “We care about our health.”
Al Richmond, executive director of Community-Campus Partnerships for Health, a nonprofit that promotes health equity, said it’s important to peel back the layers of why Black communities have higher rates of type 2 diabetes, obesity, and other chronic diseases in the first place. Ozempic and other anti-obesity drugs have quickly taken the media spotlight, but Richmond exhorts people to think about social determinants of health that contribute to chronic disease in Black neighborhoods.
For example, 1 out of every 5 Black households lives in a food desert. African Americans also face higher rates of homelessness, and areas with more African American populations are less likely to have access to green space. Richmond said any conversation about weight loss without considering these social determinants of health is missing the point.
“How do we continue to prioritize health in Black communities? What do we need to do? That’s a really complicated question,” he said. “What are the barriers that impede or drive some of these issues?”

Black bodies constantly policed
In our partner story, Word In Black interviewed 14 Black people about how they view their bodies — and 11 are women. While we reached out to dozens of Black men, it became clear that Black women’s bodies are policed, surveilled, and judged more often than anyone else.
Research shows that anti-Black and anti-fat structures in society have contributed to the distorted view society has of Black women. For example, beauty standards label Black women’s bodies as thick, too thin, or curvy. And media representation has a long history of stereotyping Black women’s bodies as deviant or hypersexual, as detailed in a 2020 journal article, “‘I’m Supposed To Be Thick’: Managing Body Image Anxieties Among Black American Women.”
“We’re living in the day and age of social media, and so many images that oftentimes paint a false narrative or reality,” Karla Robinson, medical editor at GoodRx, said about how challenging it is for Black people to have a balanced view of their bodies. “We see people aspiring to achieve an image that is airbrushed or photoshopped.”
With messages of health and weight and beauty so intertwined, Robinson said, drugs like Ozempic seem all the more tantalizing — and all the more frustrating when they are beyond reach.
Michel Hobson, a 67-year-old Texan, vehemently wants Ozempic — no matter any common side effects like nausea or even theoretically worse risks. She believes it would both help her manage her type 2 diabetes and get her closer to the idealized body images she’s encountered all her life. But Hobson is making just enough money to make ends meet and said she couldn’t possibly afford the out-of-pocket cost.
“If I could just get Ozempic, you have no idea, I’d take it in a heartbeat,” Hobson said. “Even if it meant that it would shorten my life.”
Anissa Durham is a health data reporter for Word In Black, reporting on health in the Black community.
STAT’s coverage of chronic health issues is supported by a grant from Bloomberg Philanthropies. Our financial supporters are not involved in any decisions about our journalism.
To submit a correction request, please visit our Contact Us page.




