
Around the world, patients suddenly can’t find enough of the insulins made by companies they have long relied on to do so.
In the U.S., Novo Nordisk’s recent decision to discontinue a product has left patients with fewer options. At the same time, patients are encountering shortages of other products from Novo and Eli Lilly. For months, pharmacies have been running out of vials of certain insulins that patients use to fill the pumps they wear on their body.
Supply issues have also spread to the U.K., where patients struggle to find not only vials, but also injectable pens of insulin.
And in South Africa, Novo, which had been supplying the government with human insulin injection pens for years, has stopped providing them, leading the government to alert doctors to prioritize pens for the most vulnerable.
The reasons for the shortages are complex, but the diabetes community fears one factor driving the phenomenon: Insulin manufacturers may be less interested in making it.
The histories of Novo and Lilly are deeply rooted in insulin. Novo was founded in the 1920s precisely for the purpose of creating insulin, and Lilly commercialized the world’s first insulin product around the same time. They, along with Sanofi, are the “big three” companies that dominate the global insulin market.
But in recent years, the companies have faced aggressive pressure from policymakers to lower the prices of insulin. At the same time, Novo and Lilly have discovered a massive new moneymaker — the class of highly effective GLP-1-based drugs for diabetes and obesity.
These injectable medications, which include Ozempic and Mounjaro, are so popular that the companies are frantically building and finding new manufacturing facilities to make them. They’re filled in pen devices that are similar to the pens that many insulin products come in. As demand for GLP-1s continues to climb, patients and doctors worry the companies may be turning their focus and resources away from insulin and toward the GLP-1s.
When discussing its research and development efforts, Novo “rarely” talks about insulin anymore, TD Cowen analyst Michael Nedelcovych said. “They are very straightforward when it comes to insulin’s commercial prospects, particularly in the U.S. They themselves predict continued declines, and they’ve made clear that the future of Novo’s growth is not based primarily on insulin sales.”
Insulin revenue is “effectively immaterial in the wake of incretin and novel candidate prospects,” said David Risinger, a Leerink analyst who covers Lilly, referring to the class of GLP-1 drugs.
But there will still be a population of patients who need insulin, particularly people with type 1 diabetes whose bodies don’t produce any naturally occurring insulin. These patients are concerned they’ll be left behind as Novo and Lilly go all in on GLP-1 drugs, and at the same time, they don’t know where else to turn, since Novo and Lilly have monopolized the insulin market for so long.
In a statement, Novo said it’s constantly working to optimize supply of its products to ensure patients have continuity of care. “The past couple of years have seen unprecedented changes in the market. The high level of unexpected demand along with the amount of time that it takes to establish additional manufacturing capacity are some of the key reasons behind our current short-term supply constraints,” Novo said.
When asked whether it’s shifting manufacturing away from insulin and toward GLP-1 drugs, Novo did not directly respond but said it’s “committed to improving treatment options for people living with diabetes.”
Lilly said it does not prioritize the manufacturing of GLP-1 drugs over insulin and demand for the GLP-1 drugs is not impacting its insulin supply. “We understand how vital insulin is to the people who rely on it and take our responsibility to supply these medicines seriously. Supplying and advancing insulin therapy remains a priority,” the company said.
Patients and doctors say they recognize that pharmaceutical companies are driven by financial interests and will concentrate resources on the most profitable drugs, but they also believe Novo and Lilly have an obligation to ensure continued access to the lifesaving insulin that they’ve been making for decades.
“Of course they’re more interested in GLP-1s now. Of course they are, and they want to maximize their profits before their patents run out,” said Helen Bygrave, a chronic disease adviser for Doctors Without Borders who has been monitoring the shortage of insulin pens in South Africa. “But at the same time, they have a responsibility to make sure people who need insulin continue to get it.”
Worldwide shortages
In January, Arden Parrish’s pharmacy started running out of vials of Novo’s NovoLog, a short-acting insulin that he uses to fill his pump. As the shortages extended into March, Parrish, a rising senior at Yale University with type 1 diabetes, grew anxious that he wouldn’t be able to get new vials in time, so he filled his pump with some leftover insulin that was slightly past its expiration date.
The next morning, he woke up with intense full body pain. He was extremely thirsty and had no energy to move around. It turned out he was in diabetic ketoacidosis, a severe condition in which acid builds up in the blood due to a lack of insulin. Parrish had to be rushed to the emergency room.
He’s back home in the Chicago suburbs now, and his local pharmacy still doesn’t have NovoLog vials. Parrish has instead had to extract insulin from pens of NovoLog, but the pens weren’t designed for this purpose. Several times, Parrish loaded an incorrect amount and his pump wouldn’t accept the insulin.
He’s not the only one having trouble. Parrish helps organize a mutual aid group for diabetes patients around the country, and he’s seen a surge in requests for insulin. There were already tons of requests back during the pandemic, when people lost jobs and couldn’t afford insulin anymore, but given the current shortages “I feel like we are now at or surpassed those levels,” he said.
Once an insulin is in shortage, it’s difficult for patients to switch to another option. Each person’s body responds differently to each product, and some insurance plans only coverage a narrow range of insulins.
It’s not clear why there’s been a shortage of NovoLog vials. Novo said there were “supply disruptions” earlier in the year and it has resumed shipping vials, but it may take a couple of weeks for pharmacies to fully restore their stock. Novo also said that due to an unexpected increase in demand, there is limited availability of pens of Fiasp, a faster-acting version of NovoLog, through July.
Patients also had trouble getting vials of Lilly’s Humalog for several months earlier this year. Lilly said all of its insulins are now available in the U.S.
It’s possible more patients were turning to these options after Novo and Lilly pulled other products off the market recently. Novo decided last year to discontinue an insulin called Levemir after cutting its price, and Lilly this year discontinued its 3-mL vial of Humalog, the insulin that hospitals use for in-patient care. Hospitals have now had to stock up on the 10-mL vials that patients use at home.
Lilly said it discontinued the 3-mL vials “to help create greater supply resiliency and product availability by streamlining production and distribution processes.”
Whatever the reason for the shortages, patients are frustrated by the lack of communication from the companies. Lilly put out a statement in late March saying there would be temporary shortages, but this came after patients were already having trouble filling prescriptions. Meanwhile, Novo has not said anything about insulin supply issues.

Shortages are now happening in the U.K. as well. Elizabeth Pfiester, the executive director of patient advocacy group T1International, who lives there, said that her pharmacy had been out of stock of Humalog vials since March and was only able to fill an order for vials about two weeks ago. In the meantime, she’s been attempting the tricky process of extracting insulin out of pens.
Lilly said Humalog vials are temporarily out of stock in some U.K. pharmacies due to “the dynamic nature of insulin supply and demand, coupled with a brief delay in manufacturing.”
Additionally, in the U.K., pens of Novo’s Fiasp are in shortage until at least next January, Novo said. Pens of another insulin called Tresiba are also in shortage and Novo said it expects them to return to stable supply this year.
As an indication of how tricky it can be for patients to switch to different products, the pharmacy group Community Pharmacy England issued an alert to doctors on the correct regimen that should be used when patients switch products, saying there have been reports of a few patients being advised of the wrong dosage.
Meanwhile in South Africa, Novo Nordisk has decided to not renew a contract for human insulin pens. Clinicians are now trying to transition the estimated 70,000 patients on pens to use vials and syringes instead, a much less convenient option.
Boitumelo Molema, a 22-year-old business student who was using pens, had to switch to using vials and syringes and a different type of human insulin in May. When that first happened, Molema, who has type 1 diabetes, experienced low blood sugar for two weeks, as she didn’t yet know what the optimal dosing and schedule was for her. She was fatigued and panicky the whole time.
“It’s just defeating and discouraging,” she said. “I don’t think people realize how much work goes into managing your blood sugar.”
Bygrave of Doctors Without Borders said clinicians are worried about the health system’s capacity to teach all patients how to safely measure the correct dosage from vials and inject themselves.
Novo said its decision not to renew the contract for pens was due to “manufacturing capacity limitations,” though the company is still supplying vials. Novo also noted that it’s working to expand the production of human insulin vials in Africa.
It’s difficult not to think that GLP-1s aren’t part of the reason that Novo didn’t renew the contract, Bygrave said. “There has not been a sudden surge in the demand for insulin. There has been a sudden surge in the demand for GLP-1s, which come in a very similar pen device, so — what is consuming their manufacturing line?”
A new moneymaker
Insulin is not as profitable as it once was, and it’s long been targeted by politicians vowing to lower drug prices. Just last week, the Federal Trade Commission was reported to be scrutinizing insulin makers over their negotiations with drug middlemen on prices.
Last year, a Medicaid policy went into effect that penalizes drugmakers for hiking prices higher than the rate of inflation. As a result, Novo and Lilly, along with Sanofi, all chose to lower the list prices of certain insulin products; otherwise they would have been losing money on those products for Medicaid beneficiaries.
Cutting list prices, though, meant that on the private insurance market, drugmakers weren’t able to offer pharmacy benefit managers rebates as high as they used to, so PBMs likely didn’t want to put the products on formularies anymore, reducing usage of the drugs. Novo said a factor in its decision to discontinue Levemir was a 60% decline in patient access across formularies.
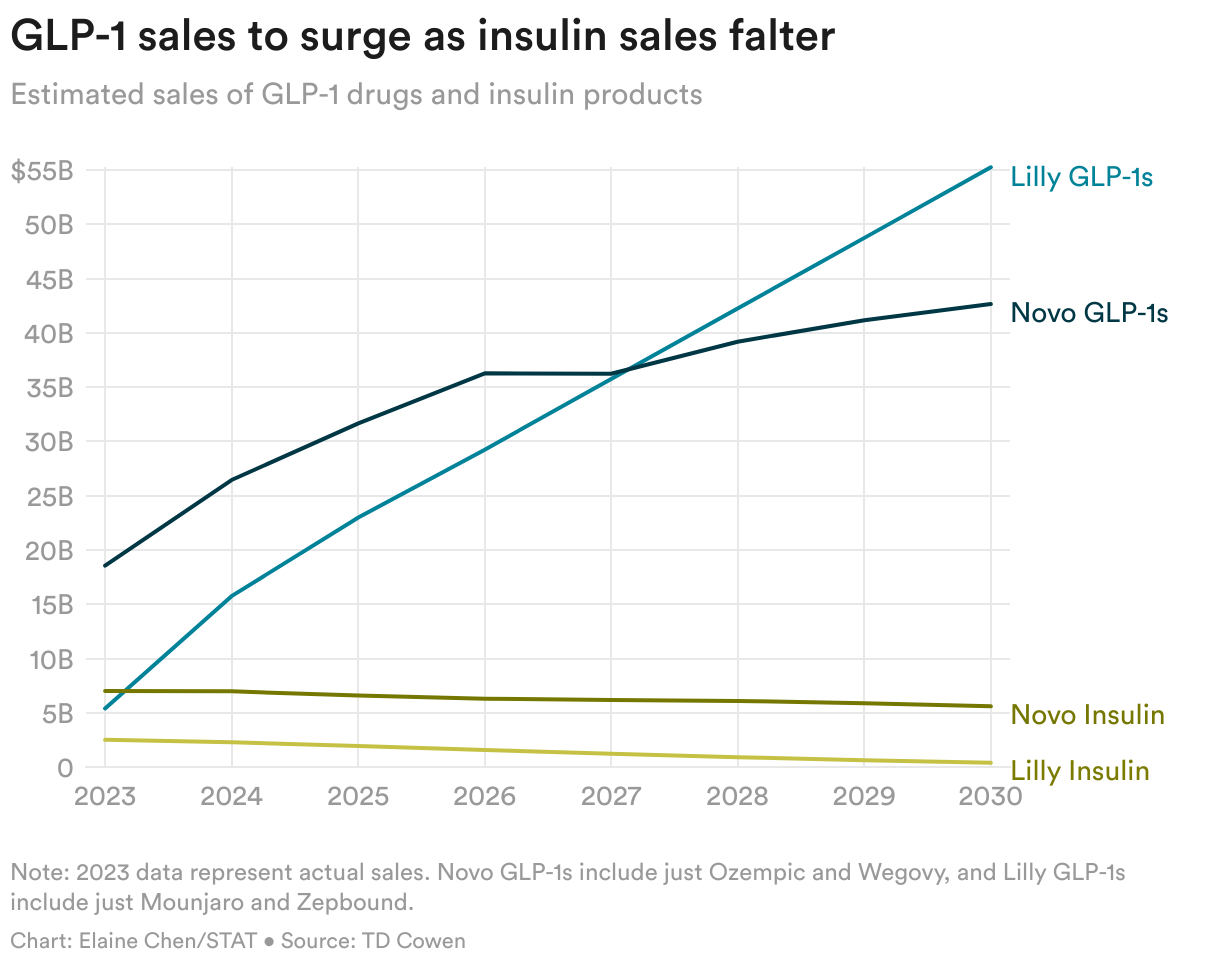
Given these pressures, analysts see decreasing sales of insulin. TD Cowen analysts predict that for Novo, sales of insulin products, not including any new products that may get approved, would drop to $5.6 billion in 2030 from $7 billion last year, a 20% decrease. For Lilly, they estimate sales to dip to $410 million in 2030 from $2.5 billion last year, an 84% reduction.
Both Novo and Lilly are developing once-weekly insulins, but these likely won’t be ideal for type 1 patients due to the risk of low blood sugar. Novo’s candidate was just rejected by the Food and Drug Administration.
Meanwhile, analysts expect sales of GLP-1s to continue to rise. Sales of just Novo’s Ozempic and Wegovy are predicted to more than double to $43 billion in 2030 from $19 billion last year, according to TD Cowen estimates. Revenues of Lilly’s Mounjaro and Zepbound are forecasted to surge to $55 billion in 2030 from $5 billion last year. These estimates don’t include next-generation GLP-1 and obesity candidates that could bring in even greater sales in coming years.
“Investors don’t really care about insulin anymore, because investors are like GLP-1, GLP-1, GLP-1,” said Emily Field, head of European pharmaceuticals equity research at Barclays. Unfortunately, for patients, “it’s still super important.”
Though the companies are for-profit businesses with a fiduciary responsibility to shareholders, some observers question whether they also have a responsibility to patients who rely on a steady supply of their medicines.
Reshma Ramachandran, an assistant professor of medicine at Yale, pointed out that the drugmakers say they’re driven by the mission of tackling serious diseases like diabetes and making medicines widely accessible. “If that mission is actually true, if they are actually going to claim this in front of policymakers, in front of patients, in front of clinicians, then yes, they do have a moral responsibility to actually ensure adequate supply and affordable pricing,” she said.
Both Novo and Lilly have said their long-term goal is to eradicate the need for insulin, and the GLP-1 drugs are in large part helping them toward that goal. As more patients get on GLP-1 drugs earlier, they argue, fewer people will progress to needing insulin.
Ramachandran said that while it’s laudable to have that goal, access to GLP-1s continues to be inequitable, meaning the diabetes patients who need them the most are not getting them and may still end up needing insulin. Additionally, type 1 diabetes patients don’t benefit from the GLP-1 drugs.
Ultimately, if the companies want to play a smaller role in providing insulin or exit the market entirely, then they should ensure that it’s easier for competitors to enter the market and that biosimilar options are “waiting in the wings ready to go live,” she said.
If the discontinuation of Levemir is any guide, that doesn’t seem likely to happen, Ramachandran said: “We haven’t seen companies taking a more proactive role to ensure that these life-saving medications are actually going to be made and continually accessible to patients.”
About the Author Reprints
To submit a correction request, please visit our Contact Us page.











