
March 5, 2024
The opioid overdose epidemic has burned through the U.S. for nearly 30 years. Yet for all that time, the country has had tools that are highly effective at preventing overdose deaths: methadone and buprenorphine.
These medicines are cheap and easy to distribute. People who take them use illicit drugs at far lower rates, and are at far lower risk of overdose or death. By beating back the cravings and agonizing withdrawal symptoms that result from trying to quit opioids “cold turkey,” methadone and buprenorphine can help people addicted to opioids escape an existence defined by drugs and achieve stable, healthy lives.
But a yearlong investigation by STAT shows that virtually every sector of American society is obstructing the use of medications that could prevent tens of thousands of deaths each year. Increasingly, public health experts and even government officials cast the country’s singular failure to prevent overdose deaths not as an unavoidable tragedy but as a conscious choice.
Narcotics Anonymous, a nationwide organization that promotes the 12-step model of addiction recovery, actively opposes the use of medication, leading would-be participants like Mark Palinski, 38, to be banned from chapter meetings in North Carolina after disclosing that he had been prescribed buprenorphine. Hundreds of jails and prisons bar their use even when prescribed by a doctor, forcing people like Amanda Cassidy-Trejo, 41, to suffer weeks of agonizing withdrawal in a San Antonio jail cell. Even specialized methadone clinics, which otherwise support the use of medications, can make them all but impossible to access, requiring patients like Rebecca Smith, 65, to show up daily at her Detroit clinic to swallow a single dose — a rule that forced her to quit her job.
Few doctors prescribe buprenorphine (commonly known by the brand name Suboxone). Roughly 40% of Walmart, Rite Aid, and CVS pharmacy locations decline to stock it. Many rehab facilities and sober living houses refuse to admit people taking either medication. Federal regulations often prevent truck drivers and pilots from taking methadone or buprenorphine. In many cases, state medical boards even prevent doctors and nurses in recovery from taking the same medications they’d provide to patients seeking treatment for opioid addiction.
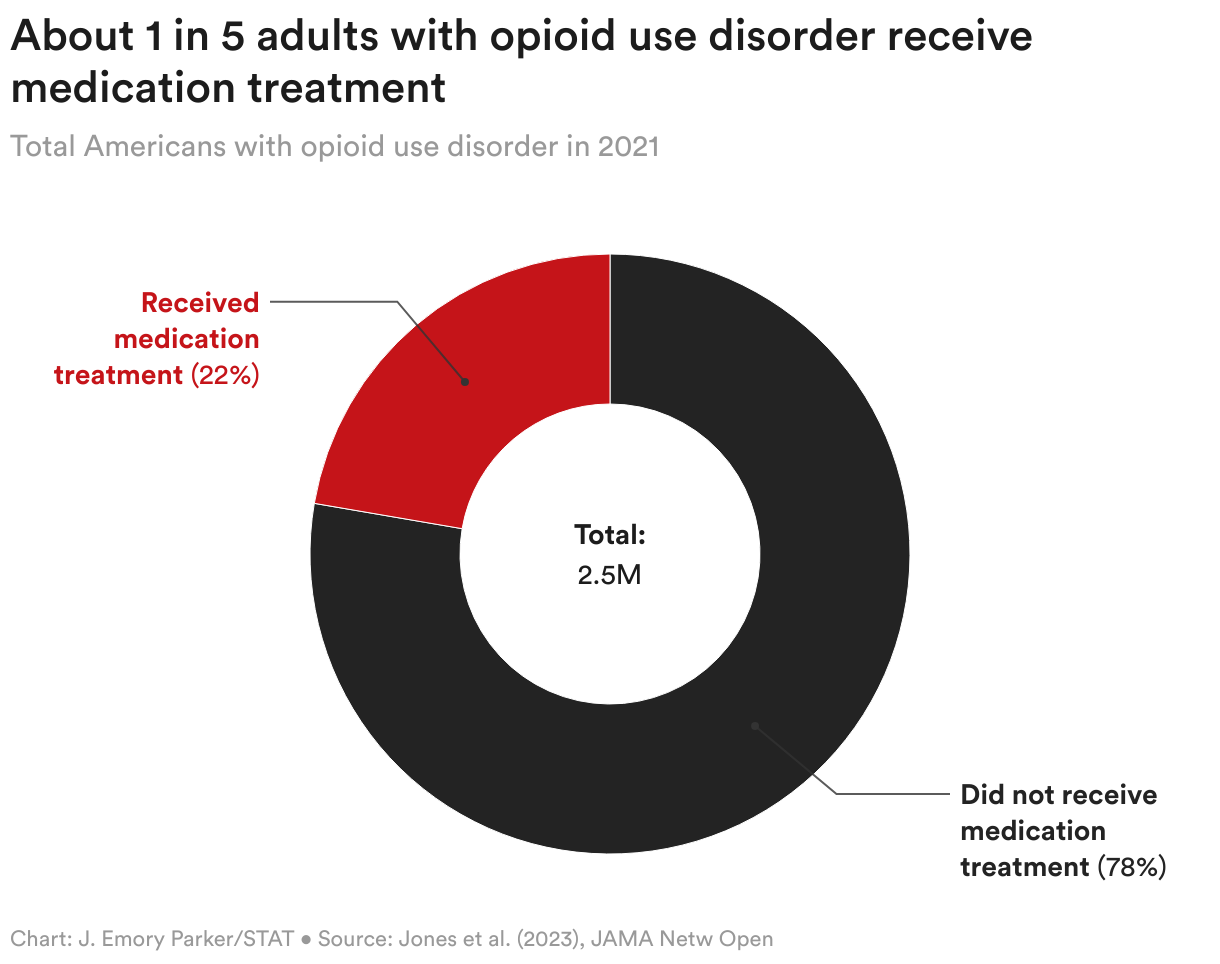
Though overdose death rates have climbed steadily for the past two decades, researchers estimate that barely one-fifth of the approximately 2.5 million Americans with opioid use disorder receive medication — and tens of thousands have died for lack of it.
“More than 80,000 people are dying of opioid overdose every year, and yet we have a tool, medication-assisted treatment, that we know dramatically reduces overdose deaths,” said David Frank, a medical sociologist at New York University who takes methadone for opioid addiction. “But because it’s so difficult to access, people that could and should be alive continue to die.”
STAT’s examination of the overdose epidemic is based on hundreds of interviews with patients, doctors, policy experts, lawmakers, scientists, and other major figures in drug policy and addiction medicine. It relies on an exhaustive review of legal documents, tax filings, financial disclosures, patient records, lobbying reports, and peer-reviewed academic research. And it includes a first-of-its-kind analysis of the ownership and practices of America’s roughly 2,000 methadone clinics, detailing for the first time how private equity firms have acquired a major stake in the nation’s addiction-treatment infrastructure while opposing calls for reform.
Methadone and buprenorphine have one major drawback: They are themselves opioids, a fact that opponents have used to cast the medications as no better than illicit drugs sold on a street corner. Indeed, they are not perfect: Methadone, which is sometimes used to treat pain, can cause sedation or even overdose if used improperly. Buprenorphine, while far safer, can also cause complications when used in combination with alcohol or other drugs. Amid a broad push to increase access to addiction medications, some experts have argued for proceeding with caution.
“We need to continue to improve access, but we need to do it in a way that maintains quality and safety,” said Kenneth Stoller, an addiction psychiatrist and researcher at Johns Hopkins University. “If we’re expanding access by just flooding the streets with a medication that we know is easily misused, and when misused is dangerous, that’s a problem as well.”
But both medications are far less potent than the illicit substances whose use they are meant to prevent, like heroin or fentanyl. And they are the gold standard for addiction treatment.
“People genuinely have no idea how effective these medications are at preventing people from dying.”
Ayana Jordan, NYU Langone Health
In an interview, Nora Volkow, the director of the National Institute on Drug Abuse, estimated that if methadone and buprenorphine were made universally available nationwide, opioid overdoses would fall by half, if not more.
“We have these very effective medications, and the question is why are they not being implemented,” she said. “I estimate that we would have at least 50% less people dying, and that’s conservative. I think it would probably be much more consequential.”
Yet instead of providing people with pharmaceuticals known to treat their condition, in the United States, common approaches to treating opioid addiction still include undergoing painful and ineffective “detox”; 12-step approaches like Narcotics Anonymous; or even “equine therapy,” a form of treatment that centers on spending time with horses.
While such programs often rely heavily on hope, mindfulness, and religion, they often ignore the physiological realities of addiction — in particular, the debilitating withdrawal that occurs when regular opioid users attempt to suddenly stop. In any other medical field, favoring prayer over proven medication would be considered malpractice. Yet for addiction treatment in the U.S., it’s simply the way things work.
“There is a core belief, that’s different from other countries, that people with opioid addiction don’t deserve care in the way that somebody who has cancer or diabetes does,” said Ayana Jordan, a researcher and addiction psychiatrist at NYU Langone Health. “People genuinely have no idea how effective these medications are at preventing people from dying.”


‘Not changing one drug for another’
The evidence supporting the use of methadone and buprenorphine is overwhelming. According to NIDA, patients using methadone and buprenorphine are 59% and 38% less likely, respectively, to die of an opioid overdose compared to those not receiving medication. Other data show an even greater effect: One recent study demonstrated an overall 80% drop in opioid overdose deaths among people taking either medication. A separate study showed that incarcerated people taking methadone or buprenorphine were 80% less likely to die of overdose in the first month after being released. The World Health Organization lists both medications on its model list of essential medicines, citing a “strong evidence base for their use.”
The medications have remarkable secondary effects, too. People being treated with methadone or buprenorphine are vastly less likely to be diagnosed with HIV, hepatitis C, endocarditis, and other diseases that can be transmitted via drug injection. Both medications are also associated with a marked decrease in depression symptoms.
While methadone and buprenorphine are opioids, they bear little resemblance to the substances that cause the vast majority of opioid overdoses — namely heroin and fentanyl. Methadone is extremely slow-acting, making it a poor option for people seeking opioids’ euphoric effects. Buprenorphine is known as a partial agonist, meaning it only partly binds to the receptor that provides a “high” when stimulated by other opioids. Practically speaking, buprenorphine only has one true use: treating opioid addiction.
A third medication, Vivitrol, has been embraced as a treatment for opioid addiction by many judges, prisons, and some doctors specifically because, though it reduces opioid cravings, it is not an opioid. A recent analysis shows that people who take Vivitrol — which costs as much as $2,100 per monthly dose — may in fact overdose at higher rates than people taking buprenorphine.
Despite the medications’ remarkable effectiveness, the country’s view of buprenorphine and methadone is built largely on myths and stigma. In 2017, Tom Price, then health secretary to President Trump, referred to what is called medication-assisted treatment as “just substituting one opioid for another.” Law enforcement agencies like the Drug Enforcement Administration, while widely criticized for allowing the proliferation of OxyContin and other painkillers that fueled the opioid epidemic in the 1990s and 2000s, now forcefully regulate buprenorphine and methadone, even as illicit fentanyl floods the market.
“They are not changing one drug for another,” said Volkow, who has led the federal government’s $1.6 billion addiction research institute since 2003. “They’re not different from other medications you may need to take, like antihypertensive medications or antidiabetic medications. They allow for your physiology to be normalized, which is necessary to achieve recovery.”
Still, in much of the U.S., the prevailing attitude remains that achieving sobriety by using medications does not constitute true recovery. Even “medication-assisted treatment,” long a common term in the field, betrays an embedded stigma: That the medication itself is not a treatment, but a supplement. Many addiction doctors now prefer a new term: medications for opioid use disorder.
In many people’s minds, the only route to beating opioid addiction is to simply stop using, experience days or weeks of agonizing withdrawal, and never use opioids again — even if those opioids are highly regulated medications prescribed for the purpose of treating addiction. Doctors, however, say the approach fails for nearly everyone who tries it, especially in the age of highly potent illicit fentanyl.
“The people that come to me to seek treatment with medication have basically all tried to stop using without medication,” said Zoe Weinstein, a doctor who serves as the director of Boston Medical Center’s addiction consult service and medical director of a methadone clinic. “There are a lot of people who need medication, and many more people who want medication than are able to access it.”

‘That’s how nuts this is’
The U.S. laws and practices governing addiction medicine are not just out of step with the latest science — they are also out of step with laws in most of the Western world.
At Arud, a substance use clinic in Zurich, Switzerland, patients receiving addiction medications are free to come and go as they please. They pick up weeks’ worth of methadone, and other powerful addiction drugs, at a pharmacy, and are not forced to undergo drug testing or regular counseling sessions as a condition of receiving their medication. While American law enforcement officials and methadone industry representatives have warned that easier access could increase methadone misuse and even overdose, Switzerland’s results have been the opposite. There, and throughout Western and Central Europe, countries that have increased addiction medications’ availability have consistently seen overdose deaths and infectious disease transmission plummet to rates vastly lower than in the United States.
“We have a precedent in France,” said Volkow, the NIDA director. “What the French did was basically provide buprenorphine to every single person that needed it. And you see this dramatic reduction in overdoses — they basically stopped.”
For decades, American physicians needed to obtain a special license known as the “X-waiver” just to prescribe buprenorphine. As of 2021, just 75,000 of the nation’s roughly 1.1 million physicians had obtained the waiver. The Biden administration effectively eliminated that requirement in early 2021, but according to data from the Centers for Disease Control and Prevention, the overall buprenorphine prescribing rate nonetheless decreased from 2021 to 2022.
Methadone, which is widely accessible across Europe, is available in the U.S. only at specialized clinics known as opioid treatment programs, or OTPs. These clinics typically require patients to report in person each day to receive a single dose, forcing them to structure their lives around the clinic’s dosing schedule.
“This is practically the only medication in the entire country that is treated this way,” said Rep. Don Norcross (D-N.J.), who has co-authored legislation that would allow specialized addiction doctors to prescribe methadone directly to patients. “The medication for abortion — that is easier accessed than methadone. That’s how nuts this is. The idea that the only way to do this is to go to the methadone clinic is just insane.”
“The medication for abortion — that is easier accessed than methadone. That’s how nuts this is. The idea that the only way to do this is to go to the methadone clinic is just insane.”
Rep. Don Norcross (D-N.J.)
The difficulty of accessing addiction medications, and the stigma that many Americans still attach to them, have deadly consequences. Studies consistently show that patients who do not take medication return to illegal drugs, overdose, or die at far higher rates than patients who do. Research also shows that as many as 90% of patients who participate in “abstinence-based” addiction treatment that bans the use of methadone or buprenorphine return to use within one year of being discharged. Treatment that relies on quitting opioids cold turkey, studies show, is significantly more dangerous than not receiving treatment at all.
Systemically denying Americans access to addiction medications has also exacerbated racial health disparities. The first decades of the opioid crisis claimed far more white lives than Black lives. But as of 2022, the trend has flipped: Black people now die of opioid overdoses at higher rates — in part because Black people seeking treatment for opioid use disorder are far less likely than white people to be prescribed an addiction medication.
The cost of these outdated and scientifically inaccurate attitudes is immense. The opioid crisis has shortened the national life expectancy by more than half a year, weakened U.S. economic output by $1.5 trillion in 2020 alone, and ruined the lives of countless others who are addicted to heroin or fentanyl but haven’t died of an overdose.
But these medications are not a silver bullet: Even if methadone and buprenorphine were universally accessible, the opioid crisis wouldn’t instantly end. Studies show that most Americans with opioid use disorder are not actively seeking treatment.
‘The system creates barriers to care’
Paradoxically, it is often those who claim to be most sympathetic to the cause of addiction treatment who are among the biggest opponents of expanded access to methadone and buprenorphine.
The recovery group Narcotics Anonymous — perhaps the country’s largest provider of addiction treatment — has taken a hard line against addiction medication. The organization’s own literature acknowledges that people taking methadone or buprenorphine are often banned from speaking at meetings, but offers a concession: “NA may be compatible for addicts on medically assisted protocols if they have a desire to become clean one day.”
In other words: In the view of Narcotics Anonymous, even people who have relied on methadone or buprenorphine to achieve stable recovery are not considered “clean.” Instead, their full participation in the program would require a pledge to stop taking medications they were prescribed by a doctor, and that first helped them quit illicit drugs.
Narcotics Anonymous did not respond to STAT’s requests for comment.
Methadone clinics have also opposed calls to expanded access to medication treatment. The American Association for the Treatment of Opioid Dependence, a trade group representing methadone clinics, has lobbied not just against the deregulation of methadone treatment, but also against a bill that passed in 2022 with overwhelming bipartisan support that made it easier for doctors to prescribe buprenorphine. And in recent decades, methadone treatment has become big business: A majority of methadone clinics now operate as for-profits, and nearly one-third are owned by private equity firms. As calls for reform have grown far louder in recent years, the methadone industry has guarded its monopoly fiercely, and remains staunchly opposed to allowing other doctors to prescribe the medication to patients in need.
Separately, according to federal survey data, at least 751 substance use treatment facilities offer treatment for opioid addiction but reject clients using methadone and buprenorphine. More than 2,000 addiction treatment facilities did not respond to the federal survey, meaning the true number of facilities banning medication is probably significantly higher.
Many medical schools still don’t require any training in addiction medicine, or prescribing addiction medications. Many hospitals still do not offer patients buprenorphine or methadone, even in the immediate aftermath of an overdose. Many pharmacies choose not to stock buprenorphine. And insurers, in an effort to pad profit margins, sometimes refuse to pay for newly developed injectable buprenorphine formulations, which last weeks or months and are shown to help patients remain in treatment — but cost far more than cheaper versions that must be taken daily.
The American criminal justice system also remains skeptical of medication as treatment. The Drug Enforcement Administration has long displayed hostility to buprenorphine and methadone, and many jails and prisons refuse altogether to provide incarcerated people with either medication. Many judges with no medical training — even in “drug court” systems supposedly meant to aid addiction recovery — have historically barred people arrested for low-grade drug offenses from taking any opioid, including addiction medications.
As workers, people taking addiction medications face immense discrimination. Many employers, labor unions, and professional societies ban their members from taking addiction medications in any circumstance.
“There are a lot of ways that the system creates barriers to care,” said Weinstein, the Boston addiction doctor. “We start to believe that if the system is created that way, it must be necessary, there must be a good reason. But that may not be true: The reason may be outdated, or never existed, or was based on stigma.”

‘It doesn’t get you high’
The addiction crisis is among the largest public health emergencies in U.S. history. But the American people and government have treated it with a remarkable lack of urgency.
Recent events provide a stark comparison. In early 2020, the Covid-19 pandemic led the U.S. to launch an unprecedented effort to develop a vaccine. The government told drug companies, in essence, that it would pay them whatever they wanted. Most doctors made clear that they would provide any eventual vaccines to anybody who wanted them.
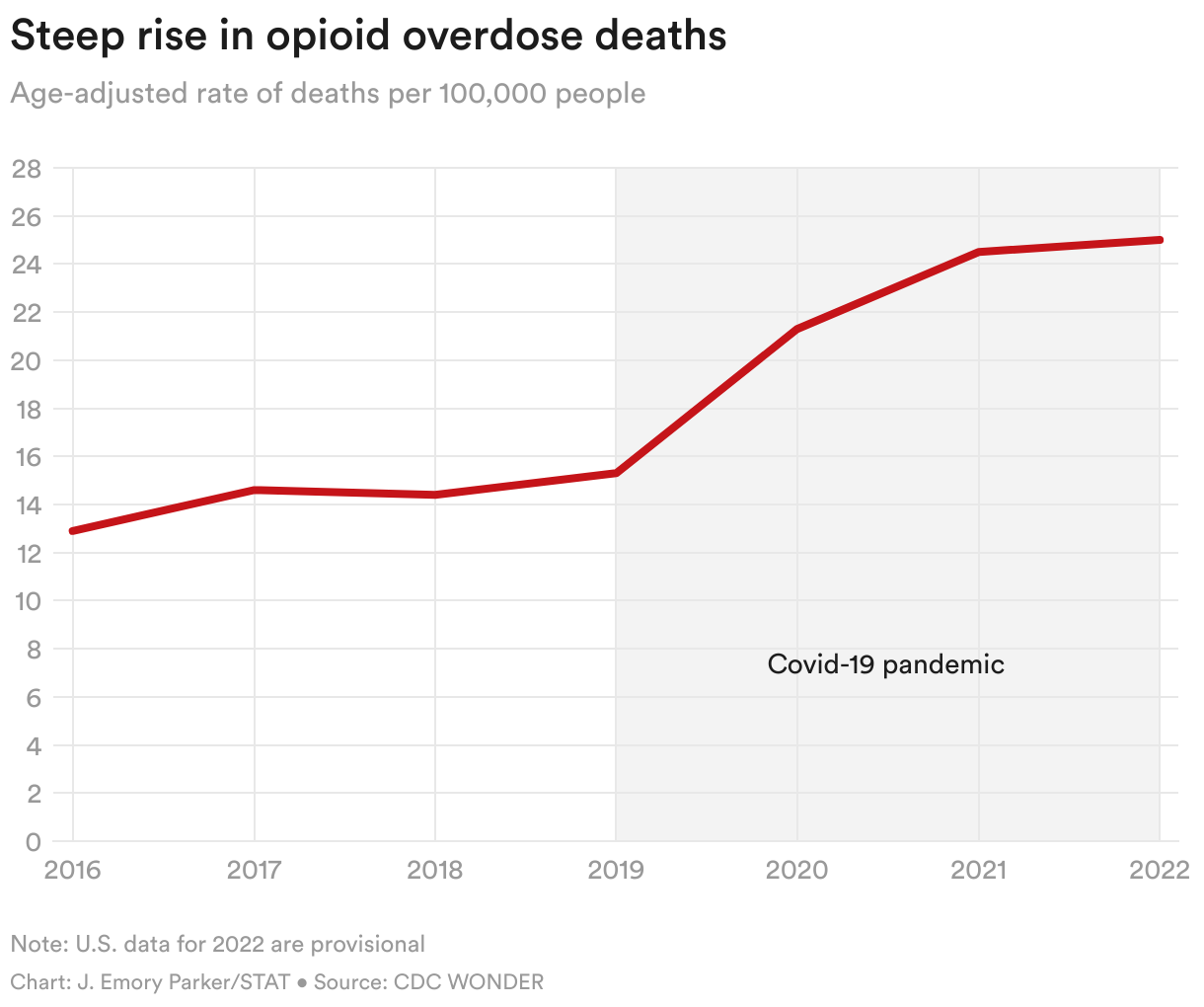
The U.S. opioid crisis is precisely the opposite. More than 1 million Americans have died of drug overdoses since 2000, and opioid death rates have steadily increased for the past two decades. But there is no Operation Warp Speed for addiction. There has been no rush to develop miraculous new drugs that can sharply reduce deaths from a devastating health crisis — in part because the government and pharmaceutical industry have displayed minimal interest in the crisis, and in part because these medications already exist.
The public’s broad opposition to addiction medications stands in stark contrast to its general acceptance of other common strategies used to improve health. Broadly speaking, Americans do not oppose drinking Diet Coke instead of Coke, cooking with olive oil instead of butter, or chewing nicotine gum instead of smoking cigarettes. But when it comes to using relatively weak, highly regulated, pharmaceutical-grade opioids to help quit deadly synthetic drugs like fentanyl, much of society remains staunchly opposed.
The entertainment industry, in particular, has often served as a cheerleader for misleading tropes and treatment approaches that oppose medication. The recent hit show “Euphoria,” for instance, depicts a teen who develops an opioid addiction but is only offered treatment based on the 12-step model offered by Narcotics Anonymous — not with medication. A decade ago, “House,” an award-winning medical drama about the star doctor at an elite teaching hospital, gave its protagonist two choices: use copious amounts of Vicodin or grit out a week of brutal and dangerous withdrawal. “Four Good Days,” a Mila Kunis movie released in 2020, is based on a nearly identical premise.
The few mainstream voices who have sought to increase acceptance for medications have failed — often in tragic fashion. Kurt Cobain, among the most influential musicians of his generation, wrote in a 1993 journal entry that he had found success treating his opioid withdrawal symptoms thanks to buprenorphine.
“The best thing about it is that there are no known side effects,” he wrote. “It acts as an opiate but it doesn’t get you high.”
The doctor who prescribed buprenorphine to Cobain died in 1993, however, cutting him off from a medication that, at the time, was only legally available as a pain treatment. Unable to find another doctor willing to provide it, he returned to heroin use. He died by suicide in 1994.



‘We need everybody to step up’
Attitudes toward medication for opioid use disorder are finally beginning to shift. The 2022 repeal of the X-waiver requirement for doctors came after years of lobbying from public health groups seeking wider access to buprenorphine.
Increasingly, researchers and members of Congress have called for ending methadone clinics’ monopoly and allowing physicians to prescribe the medication directly to patients. In 2021, the Urban Survivors Union, an activist group focused on harm reduction and the safety of people who use drugs, published the “Methadone Manifesto,” a sweeping call for change highlighting the human costs of the current methadone-distribution system.
And for the first time, the White House has pledged to make medication access a priority: President Biden said in the 2022 State of the Union address that his administration plans to make addiction medications “universally accessible” by 2025.
But there is no chance the country will meet his goal.
To do so, far more doctors would need to prescribe buprenorphine. Hospitals, pharmacies, and insurers would need to radically shift their policy and practice to encourage the use of addiction medications and provide a less hostile treatment environment for people with addiction. Congress and local lawmakers would need to pass laws mandating access to medication treatment. Branches of government including prisons, courts, and law enforcement would need to overhaul their own rules regarding access to treatment for the hundreds of thousands of people with addiction charged with, or serving time for, drug-related crimes.
Key components of the country’s existing addiction treatment infrastructure, from Narcotics Anonymous to rehab facilities, would need to adopt a different tone regarding the benefits of methadone or buprenorphine. Many methadone clinics, as well, would need to take a more welcoming, less punitive tack toward patients who come to seek treatment.
Absent those changes, American society’s deeply embedded bias against addiction medications make it all but certain that the status quo will remain — or at least, that the U.S. won’t change course before losing hundreds of thousands more of its citizens.
“Outdated views, combined with stigma around treatments for opioid use disorder, combined with the challenging regulatory environment, are leading to a situation where people just aren’t getting evidence-based care,” said Jesse Ehrenfeld, an anesthesiologist and president of the American Medical Association. “This is a moment where we need everybody to step up, and stop dragging their feet.”
STAT’s coverage of chronic health issues is supported by a grant from Bloomberg Philanthropies. Our financial supporters are not involved in any decisions about our journalism.
Do you have an experience with medications for opioid use disorder? Share your story with STAT
Story Credits
Reporting, data gathering and analysis: Lev Facher
Graphics and data analysis: Emory Parker
Video reporting: Alex Hogan
Editing: Laura Chang
Art and photo direction: Alissa Ambrose
Photo editing: Crystal Milner
Illustration: Thumy Phan
Additional editing: Rick Berke, Gideon Gil
Copy editing: Sarah Mupo and Karen Pennar
Design and development: Jennifer Keefe, Julia Bujalski, Ben Lokshin
About the Author
To submit a correction request, please visit our Contact Us page.





