Researchers were perplexed when the Food and Drug Administration announced it was investigating whether CAR-T therapy, one of the most effective treatments for blood cancers, could cause lymphoma. This was always a theoretical risk of genetically engineered therapies like CAR-T, but it never materialized in the decades after the technology’s birth.
So, when the agency pointed late last year to a couple dozen cases of T cell lymphoma in patients who had previously been treated with CAR-T cells, it felt like an old question had been reignited. The field jumped to investigate whether CAR-T truly could cause new cancers — and what the odds were if so. Those efforts have led to a “flurry of publications,” said Marcela Maus, a CAR-T researcher at Mass General Cancer Center.
These studies have helped to answer “some of the questions that were precipitated by the FDA announcement,” Maus said. They still have not found definitive evidence that CAR-T therapy has directly caused new cancers, she said, and scientists continue to suspect that such an event would be extremely rare.
While the FDA is continuing to gather information, it is for now asking patients be monitored lifelong for second cancers, and for clinicians to report any suspected emergence of secondary malignancies. The agency is also requiring boxed warnings for CAR-T therapies, to make patients aware of the rare complication of a secondary cancer.
What the recent papers do is give scientists a better idea of how often CAR-T patients go on to develop any subsequent malignancy, Maus said, and provide a blueprint for how clinicians might be able to detect the development of a potential CAR-T-induced cancer. “It gives an outline of what the work up can be,” Maus said. “So that people can follow up and identify the smoking gun. Tell us if you find it.”
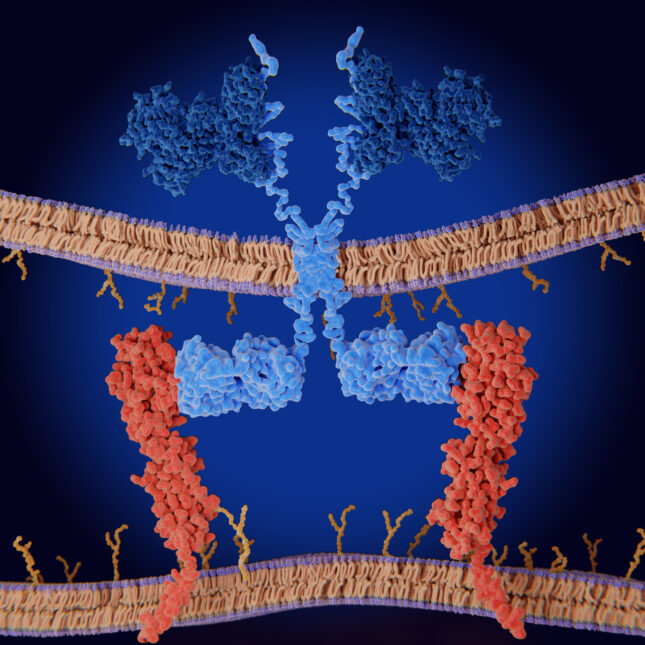
The main hypothetical concern centers around the genetic editing method used to create the therapy. CAR-T cells are genetically edited T cells that carry a synthetic protein called a chimeric antigen receptor or CAR, which helps these immune cells recognize and kill cancer. The six currently approved CAR-T products use a modified virus that delivers the CAR gene into the cell’s genome, but the problem is that these viruses don’t integrate these genes in a perfectly precise way.
Theoretically, the CAR gene could get accidentally slipped into the middle of some other, crucial gene, like one that controls cell division or DNA repair for example, and break its function. That kind of mutation could kick off the formation of a new cancer.
Because CAR-T production only edits T cells, researchers first focused their attention on T cell lymphomas. If the CAR gene strayed into a cancer-causing mutation, then that gene should show up as a kind of fingerprint on every cancer cell. In two reported cases so far, one published in Blood and another published in the New England Journal of Medicine, scientists found T cell lymphomas in patients previously treated with Janssen’s Carvykti, a CAR-T treatment for myeloma, which carried the CAR gene.
But when the researchers looked more closely, the CAR gene didn’t wind up in places associated with cancer formation in either case. In the case published in NEJM, the CAR integration did affect a gene related to T cell maturation, but it didn’t seem to have any great impact on the cells, said Metin Ozdemirli, a pathologist at Georgetown University and the lead author of the study. “The integration site is very interesting,” he said. “Loss of that change can cause CD4 T cells to become cytotoxic, but we looked at RNA expression of this gene. We didn’t see abnormal expression.”
That suggests, at least in these two cases, that it wasn’t the CAR-T manufacturing that created these patients’ T cell lymphomas. So, what did?
“The more likely scenario is that these patients already have higher inherent risk due to many factors, such as prior therapies,” said Kai Rejeski, a cancer researcher at Memorial Sloan Kettering Cancer Center.
In general, cancer patients are already at higher risk of getting another, unrelated cancer. One reason is that many cancer therapies, like chemotherapy, radiation, and some targeted therapies, increase the chances of getting a subsequent malignancy. CAR-T patients have tended to have an exceptionally high burden of this, as CAR-T has historically been given only as a late line therapy.
Blood cancer patients also may have a higher burden of cancer-related mutations. Oncology researchers Ash Alizadeh and David Miklos noticed this when they investigated second primary malignancies in over 700 patients treated with CAR-T at Stanford University. One patient initially treated with CAR-T for a B cell lymphoma went on to develop a second T cell lymphoma after the therapy — but she also already had two mutations in her blood stem cells that likely predisposed her to independently developing both of these cancers.
“This tumor blossomed while [the other] shrank, but the seeds of it were in her body before the tumor developed,” Alizadeh explained.
These factors also predispose patients to many other kinds of cancers, not just T cell lymphoma. Alizadeh’s study, along with others, suggest that about 7% of CAR-T patients develop any subsequent malignancy after a few years. That’s more than is seen with just chemotherapy, which can lead to new cancers about 1% of the time, but patients usually have gone through many rounds of treatment by the time they get to CAR-T. Patients who get bone marrow transplants similarly go through multiple rounds of treatment, and the rate of subsequent cancers in this group can range from 10% to 20%, depending on the length of follow-up, said Memorial Sloan’s Rejeski.
There are also some hypothetical reasons why CAR-T could indirectly raise the risk of any secondary primary malignancy, Rejeski added. For one, CAR-T therapy can cause inflammatory proteins to reach dangerous levels in the body, and physicians manage this using immunosuppressive drugs. CAR-T therapy also lowers certain immune blood cell counts in the body. That might play a speculative role in allowing pre-malignant cells to grow out of control. “But that’s hypothetical,” Rejeski said. “We’re lacking randomized trials looking at if this is truly facilitated by CAR-T therapy.”
In any case, the risk of subsequent malignancies after CAR-T therapy is relatively low. Patients develop T cell lymphomas after CAR-T therapy extremely rarely — less than 0.1% of the time, Rejeski said. Second cancers also rarely cause death in CAR-T patients, Rejeski said. Mortality from these subsequent cancers occurs roughly 0.5% of the time. In comparison, infections led to the deaths of about 4% of CAR-T patients in a study that Rejeski published in Nature Medicine this week. “Infections, infections, infections. This is the main driver of non-relapse mortality,” he said.
That suggests that while these risks should be taken seriously, it’s still the case that CAR-T therapy’s benefits “for the vast majority of patients far outweigh the risks,” said David Porter, an oncologist at the University of Pennsylvania School of Medicine, who contributed to the first decade-long study that showed leukemia remission in two patients.
Considering that CAR-T is often one the last lines of therapy for patients, Rejeski pointed out, the choice is often between accepting the risks of CAR-T or dying of the cancer you have.
While the overall picture of CAR-T’s safety has not changed, the FDA’s expression of concern is helping researchers make the therapy even safer by learning more about its complications. “That’s teaching us to do better,” Rejeski said. “And how we can further improve outcomes.”
About the Authors Reprints
To submit a correction request, please visit our Contact Us page.











